M. tuberculosis (TB): From “Sexy” to Stigmatized
Key Takeaways
Tuberculosis (TB) has existed for thousands of years. In parts of Europe, it was once romanticized and even considered beautiful before becoming associated with poverty and racial inferiority.
The way we talk about diseases like TB, HIV, and COVID-19 reflects social bias as much as biology.
Illness feels personal. But it is deeply social.
TB
Tuberculosis has been with us for a long time.
Ancient Egyptian skeletons show spinal deformities consistent with TB. In ancient Hebrew texts, a “wasting disease” appears in scripture. The Greeks called it phthisis.
Tuberculosis is not new. It has walked alongside humanity for millennia.
And yet, the way we understand TB has changed throughout the years.
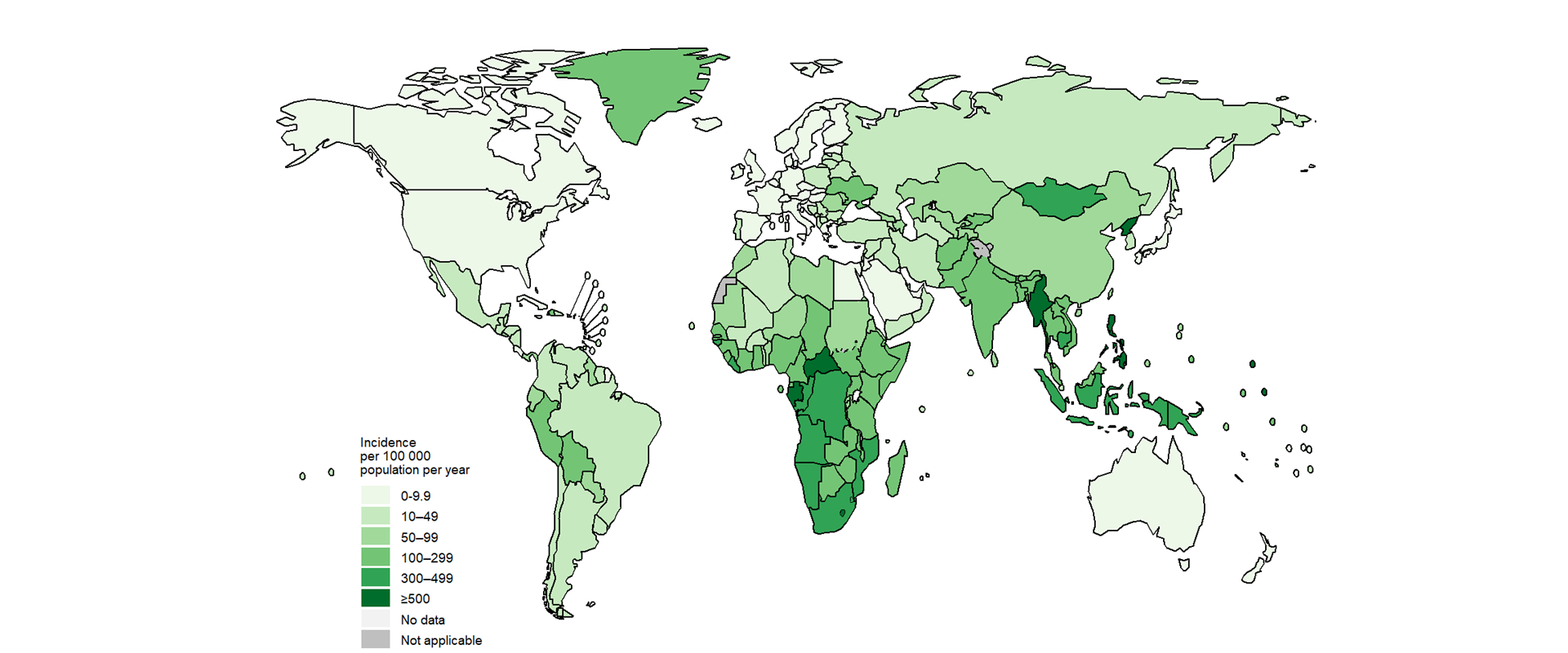
(Global Burden of New TB Cases- 2023)
Today, over 80% of TB cases and deaths occur in low- and middle-income countries like Pakistan, India, Nigeria, and the Democratic Republic of Congo. TB is the single most infectious disease worldwide and other than at the peak of the COVID-19 pandemic, it has the most infectious disease fatalities in its cache.
It’s preventable.
It’s treatable.
But treatment is long. Six months at minimum. Sometimes a year or more. And if treatment is interrupted, the bacteria get smart. Multidrug-resistant TB develops and infection learns how to survive.
Then, there’s the harsh truth that
Where the cure is, the disease is not.
And where the disease is, the cure is not.
Think about when your mom said, as insensitive as it might feel now, “There are starving kids around the world who would love the food you have,” and you still tossed those greens.
In America, we have too much food, while those who need it most—to combat malnutrition—are stuck in systems of ethnic cleansing that prohibit food (and aid) from entering. Treatment for TB is the same. Those who need it the most have limited access to that need. TB now sits as an infection among the poor and most disenfranchised people in the world. But this wasn’t always the case
Today, I want to share something I learned from John Green’s most recent book: Everything is Tuberculosis.
Yes—that John Green. The one who could write to a 12-year-old girl’s heart like no other. The Fault in Our Stars. Looking for Alaska. Paper Towns. This is also the John Green who hosted my favorite YouTube channel: Crash Course.
He wrote a great book about tuberculosis but I’ll provide a brief summary of what I found most interesting. Green dedicates about two chapters to outlining the moment TB shifted from a socially desirable, even coveted illness to an infection associated with the poor, illiterate, and racially inferior.
When TB was “Beautiful”
Before it was called tuberculosis, it was called consumption because of the way it consumed the very life essence of the living.
And at one point, especially in Western Europe, consumption was… romantic.
The symptoms were aestheticized. They fit the beauty standard of the time.

Pale skin. Flushed cheeks. Thin frame. Bright, glassy eyes.
(See: Eliza Poe- Edgar’s mom)
Consumption during Poe’s time was viewed as an inherited disease of more sensitive and beautiful souls- like women and artists. Consumption was desired among men as well. Dying from the disease was understood as a rarity (even though basically everyone had it) and something noble.
Lord Byron, famous poet but more famous socialite playboy, once said:
“I should like, I think, to die of consumption… because the women would all say, ‘see that poor Byron- how interesting he looks in dying!”
They think he died of malaria…
Other famous victims of consumption include:
· John Keats: a famous poet
· The Bronte family – Wuthering Heights, Jane Eyre
· Frederic Chopin, the musician
Poets wrote about fever like it was poetry itself.
See how Anne Bronte wrote about her sister Charlotte wasting away from TB:
“Consumption, I am aware, is a flattering malady.”
And Keats
“O what can ail thee, knight-at-arms
Alone and paley loitering
….
I see a lily on thy brow,
With anguish moist and fever-dew
And on thy cheeks a fading rose
Fast witherth too”
The conclusion: Before 1882, consumption, in parts of Europe at least, was sexy. Consumption was a refined, noble and beautiful way to die.
Then came Robert Koch, who identified Mycobacterium Tuberculosis in 1882 as an infectious agent. M. tuberculosis, no longer poetic, is now contagious. No longer the inherited trait of delicate, artistic white beauty, it became associated with overcrowding, poor sanitation, and “moral and racial inferiority.”
See below how this was documented by a 19th century American doctor:
“The negroes of Georgia, and I might say of the Southern States, up to 1860 enjoyed remarkable mental and physical health, and they were almost entirely exempt from certain diseases to which they are now not only very susceptible, but are dying much more rapidly from these maladies than the whites; namely, insanity and consumption.”
In more overtly racist fashion, another doctor wrote in “The Susceptibility of the Negro to Tuberculosis” to claim that enslaved people were wholly exempt from TB, implying that freedom made them ill:
“Before the war between the States, when the negro was a slave, tuberculosis was exceedingly rare, and some observers regarded [the negro] almost, if not quite, immune.”
Let’s Pause.
Black people did not suddenly start contracting TB once the Emancipation Proclamation was signed.
It could be very possible that those considered 3/5ths of a person would be given little study or concern should they begin coughing up blood. Formerly enslaved people were pushed into overcrowded housing, denied medical care, and excluded from resources like rest, nutrition, and sanatorium treatment. The disease patterns reflected living conditions.
TB “became” an infectious disease and society blamed race… we blamed Black bodies rather than address systems that killed them (sound familiar?).
The same pattern showed up in residential schools for Indigenous children in Canada. With overcrowding, malnutrition, neglect, TB spread rapidly. The conditions weren’t accidental. The neglect of native children in these school led to higher rates of infection and death from TB which, as I told yall, is preventable.
TB shifted from:
a romanticized “white” inherited frailty
to
a stigmatized disease of the poor, the racialized, the “inferior.”
The bacteria did not change.
The story did.
Note: What I’ve written so far has come from a Eurocentric stand point (what doesn’t…..when will I be freeee??) but it is interesting to note that counties like India and China, while not having the scientific name of M. Tuberculosis, had long recognized TB as something that can spread from person to person.
While I love history, I want to pause here to think about how a disease that once made people look “interesting” became a sign of moral and social failure. TB, while a great case study, isn’t the only illness that’s gone through this kind of shift in social understanding.
Most recently, the COVID-19 infection went from being a racialized and shamefully entitled “Chinese flu” (by y’alls President) to a campaign to protect mee-maw by wearing a mask. The HIV/AIDs epidemic, once labeled the gay disease, still largely burdens men who have sex with men (MSM) but in 2021 60% of new HIV cases among women were found among African American women.
And then there’s class.
The other day I got a $300 medical bill- and I took my $300 and paid my car insurance. That was my choice.
For someone else, that $300 might mean choosing between groceries and medication.
You think millionaires are making those decisions?
Healthcare access shapes who gets sick, who gets treated, and who comes out alright on the other side.
Illness, while an individual experience, is deeply social.
Humor me if you will: Close your eyes. (But also, don’t. You’re reading)
Just pretend your eyes are closed.
For each illness below, think about the type of person you visualize
Cancer?
A child with cancer?
Breast cancer? Colon cancer? Liver or lung?
Type 1 diabetes?
Type 2 diabetes?
(Need to know the difference? Here you go: https://www.diabetes.org.uk/diabetes-the-basics/differences-between-type-1-and-type-2-diabetesLupus?
Leprosy?
Malaria?
HIV?
Who do you picture?
Be honest.
Most of us visualize specific kinds of people. Certain races. Certain ages. Certain lifestyles. And maybe you’re pretending you notice no pattern in the people you visualize. Congrats you’ve convinced yourself you have no bias.
But one thing is certain- disease doesn’t exist in a vacuum. It’s not just about biology. And who we “expect” to carry it can change. Disease shapes the places we live in, the way we speak about sickness and healing and even in what we see as “sexy”.
In reality, here is nothing sexy about a fever. Nothing romantic about coughing up blood. Nothing aesthetic about wasting away.
But what is it about the feverish tinge of blush on my cheeks that makes me feel more delicate… more feminine?
I’m still learning how to unlearn my own assumptions about health, worthiness and care. As someone working in public health, that feels non-negotiable.
If there’s one thing I hope you take from this, it’s this:
TB didn’t change.
The story we told about it did.
And stories shape everything.
Thank you, John Green, for always teaching this girl something new.
I wrote it down so we can learn it together,
-Kiara
There will be no APA format- this ain’t for a grade. Click the links if you wish:
1. https://pmc.ncbi.nlm.nih.gov/articles/PMC5432783/#R14
2. https://www.who.int/news-room/fact-sheets/detail/tuberculosis
3. https://www.abdn.ac.uk/media/site/pgrc/documents/Granite_Tuberculosis.pdf
5. https://jamanetwork.com/journals/jama/article-abstract/455538#
6. https://pmc.ncbi.nlm.nih.gov/articles/PMC2262517/?page=2
7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9930508/